Home
Services
About us
Blog
Contacts
Vet App Development 2025: A Practical Playbook for PIMS Integrations, Telemedicine Compliance and AI-Ready Mobile Workflows
1.Market Map 2025: Where Vet App Development Meets PIMS, Labs, eRx, Insurance & Payments
2.Regulatory Fit by Design: US VCPR, UK RCVS “Under Care,” and Safe Telemedicine Flows
3.Architecture Blueprint for Vet App Development: Mobile ↔ PIMS Data Spine, Offline-First Sync, Security & Audit
4.Features That Move the Needle: Client App, Staff App, Telemedicine, eRx, Claims, Imaging/PACS & AI Scribe—Prioritized by Outcomes
5.Delivery & TCO: Integration Playbooks, SLOs, and a Cost Model You Can Reuse
6.Build-to-Scale with A-Bots.com: Engagement Models, Case-Style Patterns & a Vet App Development RFP Checklist

1.Market Map 2025: Where Vet App Development Meets PIMS, Labs, eRx, Insurance & Payments
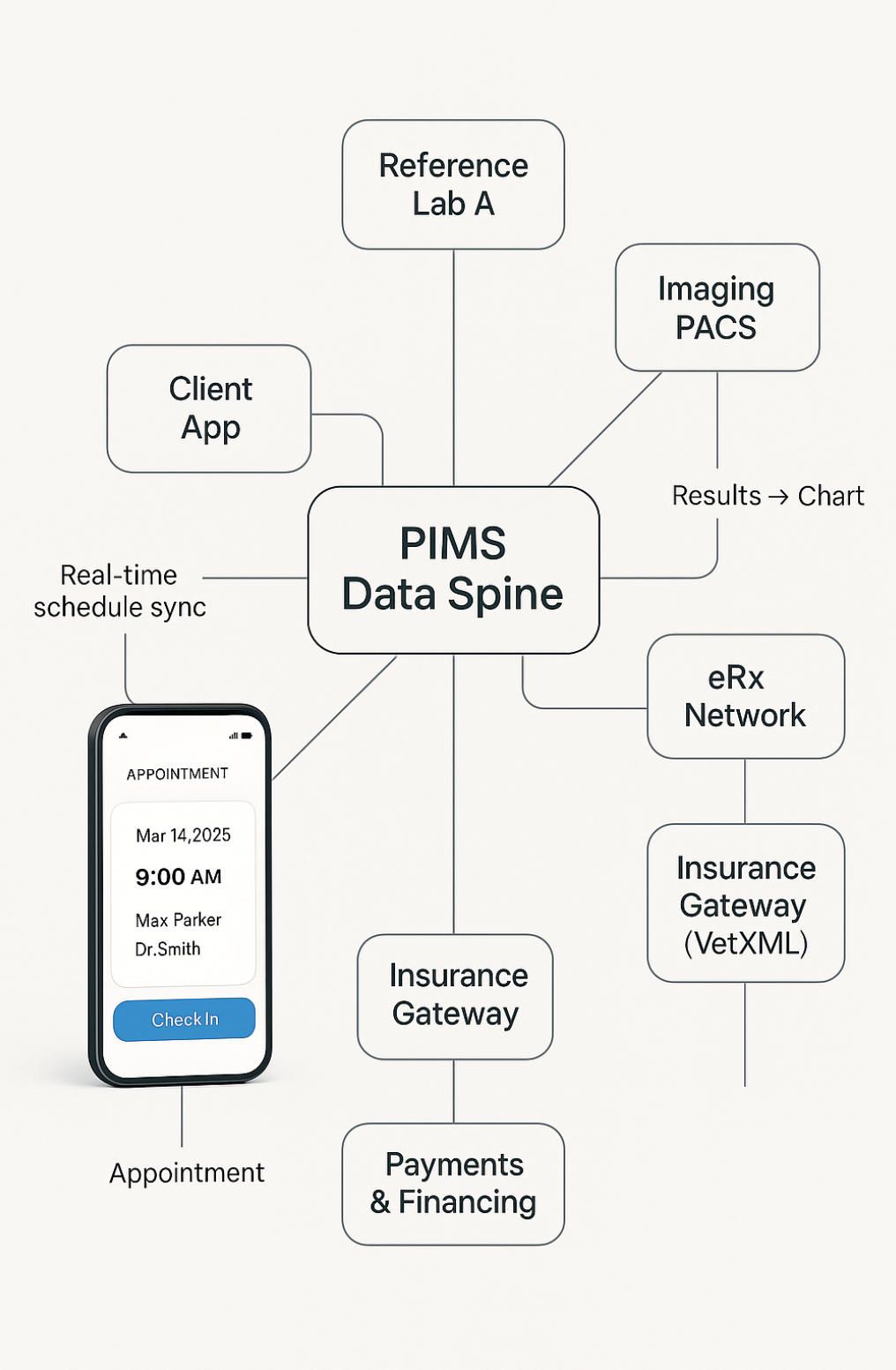
If you’re serious about vet app development in 2025, you’re not building a standalone mobile UI—you’re docking a mobile workflow into a crowded, evolving ecosystem: PIMS backbones, lab & imaging rails, e-prescribing networks, client-engagement layers, claims, payments, and jurisdiction-specific constraints. The map below shows what “plugging in” actually means and where a custom app can create outsized leverage.
PIMS first: the data spine you must respect
The majority of real-world workflows (appointments, SOAP, charges, inventory, reminders) live inside a Practice Information Management System. A workable vet app development plan starts by choosing target PIMS and their integration paths:
-
IDEXX stack (Cornerstone, Neo, ezyVet). This family sits at the center of many North American clinics and offers a large integration surface—diagnostics, Web PACS, payments, and booking partnerships—exposed through curated partner endpoints and connectors. For example, ezyVet advertises packaged integrations with IDEXX VetConnect PLUS (reference labs) and Vetstoria (online booking with real-time schedule sync). software.idexx.com
-
Provet Cloud. Public REST API + webhooks make it attractive for event-driven mobile apps: create/consume encounters, subscribe to updates, and reconcile offline edits safely. developers.provetcloud.com, support.provet.cloud
-
Vetspire. API-forward cloud PIMS with AI features; its developer docs formalize tokened read/write access to practice data—relevant for robust mobile CRUD and background sync. developer.vetspire.com, vetspire.ai
-
Digitail & client app. “All-in-one” PIMS plus a pet-parent app (appointments, chat, telemedicine) that your custom front end may complement or replace in specific journeys. Digitail
Why it matters: without a PIMS-aware data model (patients, encounters, orders, charges, comms), mobile apps become “double entry” tools and die in production. A-Bots.com ships PIMS adapters and event translators as part of discovery so features land where teams actually live: inside PIMS.
Client engagement & booking: where attrition hides
Owner-facing convenience (24/7 booking, reminders, two-way messaging) is now a retention moat. PetDesk’s 2025 study reports 31% of pet parents are considering switching vets—digital convenience gaps are a key driver; clinics not offering reminders, self-service booking and seamless records access are losing share. Vetstoria’s direct PIMS sync (e.g., ezyVet) eliminates double-booking and exposes rule-based slots to the web. PR Newswire, PetDesk, Vetstoria
Implementation note: in vet app development, build your booking layer to honor PIMS scheduling rules (slot length, provider type, visit reason) and to degrade gracefully when a clinic prefers an external scheduler (e.g., Vetstoria) that still writes back into the PIMS. Pet-parent apps (PetDesk, Digitail) are competitors and partners at once; design for coexistence via webhook/event handlers. PetDesk
Labs & diagnostics: orders, results, and the “turnaround loop”
Most clinics rely on reference labs (IDEXX, Antech, Zoetis) and in-house analyzers. Good vet app development supports lab orders/results without retyping codes, and it ties charges to orders to avoid leakage.
-
IDEXX VetConnect PLUS. Deep ties to ezyVet/Cornerstone/AVImark; test ordering and result injection into the patient record, plus mobile notifications. ezyvet.com, Covetrus.com, idexx.com
-
Antech. Documented ezyVet integration for catalog sync and automated result return. docs.ezyvet.com, ezyvet.com
-
Zoetis Reference Labs. 2025 expansion with a new Louisville, KY reference lab co-located at UPS Healthcare Labport to accelerate nationwide sample logistics—shorter specimen-to-result cycles you can surface in app SLAs. news.zoetis.com, lanereport.com
Imaging/PACS. Expect DICOM viewers inside clinician/staff apps. ezyVet embeds links for IDEXX Web PACS and integrates with third-party PACS such as VetRocket (RocketPACS), while Covetrus Pulse now lists RocketPACS integration. Build viewing and annotation that deep-links back to the PIMS chart.
eRx & pharmacies: align UX with real networks
e-prescribing and pharmacy orchestration are becoming standard in vet app development:
-
Vetsource Prescription Management. Unified Rx creation/approval, retailer requests, AutoShip, reporting, mobile-friendly flows; integrations minimize re-entry and maintain complete pharmacy history in the chart. Vetsource, help.vettersoftware.com
-
Covetrus vRxPro. Next-gen Rx management integrated with major PIMS; synchronized orders and treatment recommendations feed the medical record. Covetrus.com
-
Surescripts + ScriptSure (DAW Systems). Announced 2024 expansion to veterinary medications via the national eRx network—important when your app targets retail pharmacy fulfillment outside the practice. Surescripts, dawsystems.com
Compliance guardrails: regardless of state experiments, at the federal level a VCPR cannot be established solely via telemedicine; design your flows to enforce in-person prerequisites before certain prescriptions (and expose “advice-only” or refill-eligibility states in the UI). U.S. Food and Drug Administration, avma.org
Insurance & claims: UK is codified, US is an opportunity
In the UK, VetXML/VetEnvoy standardize e-claims from PIMS to insurers with status tracking; many UK PIMS integrate this directly, reducing admin time and accelerating payouts—some vendors cite 3–4× faster settlement once e-claims replace paper. For US clinics, there’s no dominant equivalent yet—room for a claims “thin layer” in your app. VETXML, software.idexx.com
The UK’s Competition & Markets Authority is pushing remedies for transparency (pricing, medicines, plans), pushing the market toward digital disclosures your app can automate (clear prices, plan terms, Rx options). Expect rules to crystallize in late-2025. GOV.UK
Payments & financing: from checkout friction to conversion
Integrated payments are now expected in PIMS (IDEXX offers integrated processors across Cornerstone/Neo/ezyVet), enabling links by SMS/email and faster closeout. For high-ticket care, CareCredit (accepted at 27,000+ US practices) and Scratchpay offer financing rails that your app should surface pre-treatment with soft checks and cost clarity. Tie approvals to treatment estimates and reduce counter-surprises.
Interoperability: FHIR exists for animals, but VetXML “wins” in UK admin
HL7 FHIR includes a patient-animal extension (species, breed, reproductive status) that you can use to structure exports and owner-facing records; the UK’s VetXML remains the lingua franca for e-claims and some admin exchanges. A practical vet app development program supports PIMS APIs today, emits FHIR for portability, and maps VetXML where claims matter.
What this means for your roadmap
- Treat PIMS + labs + eRx + payments as first-class “systems of record”; your mobile UX should be a latency-tolerant cache, not a forked database.
- Bake in jurisdiction-aware telemedicine: advice-only flows, refill rules, and hard stops when VCPR preconditions are unmet.
- For the UK and any insurer-heavy market, add claims status and document packs (VetXML today; design for US variants tomorrow).
- Use event webhooks (e.g., Provet Cloud) to drive real-time updates and reliable offline sync queues.
A-Bots.com builds these layers as reusable integration playbooks—PIMS adapters, lab/eRx connectors, offline-first sync, and compliance guardrails—so your vet app development starts from a production-tested spine rather than a greenfield experiment.
2.Regulatory Fit by Design: US VCPR, UK RCVS “Under Care,” and Safe Telemedicine Flows
In vet app development, compliance is not a footnote—it’s the spine of your product. The fastest way to ship risk is to treat telemedicine like a generic video chat. The right way is to encode jurisdiction-aware rules into UX, data models, and integration contracts so that every screen either enables or prevents a clinical action by design.
The two big regimes your app must honor
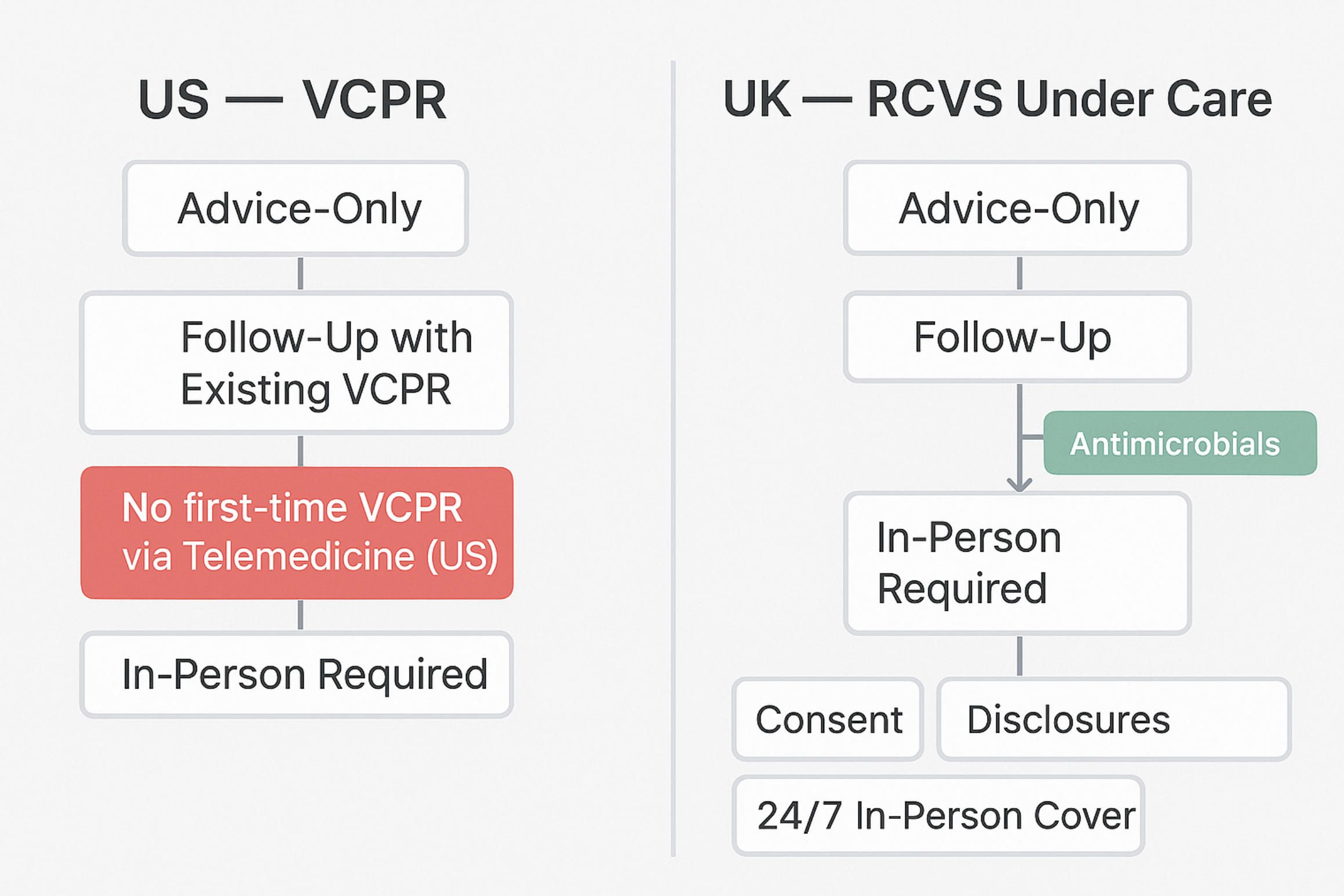
United States (federal + state patchwork). At the federal level, the FDA’s Center for Veterinary Medicine requires a valid VCPR for extralabel drug use and Veterinary Feed Directives; critically, a VCPR cannot be established solely via telemedicine. You can maintain an existing VCPR remotely, but you cannot create it by video/audio alone—period. States then add their own definitions and allowances on top of this federal floor, which is why a state-by-state switchboard is mandatory in production apps.
United Kingdom (RCVS “Under Care”). Since 1 September 2023, the RCVS allows remote prescribing after a clinical assessment, and whether that assessment must include a physical exam is generally the vet’s judgement—with explicit exceptions: antimicrobials, antifungals, antiparasitics, antivirals, notifiable diseases, and (in practice) controlled drugs typically require a physical exam at the time of prescribing. “Under care” also implies 24/7 capability to provide in-person follow-up (directly or via arrangements). Your app must surface these guardrails at the moment of intent, not in a policy page. Professionals
Product rules that should be hard-coded (not left to chance)
1) Jurisdiction detection and gating. Resolve the owner’s and practice’s locations up front; lock telemedicine flows accordingly. In the US, block “first-time VCPR by video” and steer to in-clinic booking; in the UK, allow remote prescribing unless the medicine class triggers a physical exam requirement (auto-gated by Rx class). Maintain a living state ruleset using authoritative sources (e.g., VVCA’s map; AAHA/AVMA guidance).
2) Role-aware clinical actions. Make “advice-only” and “triage” first-class actions distinct from “diagnose & prescribe.” In US states that permit teletriage without VCPR, mark outputs explicitly as advice and suppress any eRx UI. Where a VCPR exists, unlock eRx but still apply drug-class checks and dosage/refill limits per local law. avma.org
3) Medication-class logic (UK). If a clinician selects an antimicrobial/antiparasitic/antiviral or a controlled drug, require confirmation of a same-time physical exam (or documented exception) before enabling “Sign & Send.” Store justification text in the clinical notes automatically. Professionals
4) WORM audit & consent rails. Every telehealth action (advice given, triage outcome, refusal to prescribe, redirect to in-person, Rx attempt blocked) should hit an append-only audit stream. In the UK, pair this with price/plan disclosures—CMA’s 2025 remedies push the sector toward transparent pricing and options, so build disclosure surfaces now.
5) Claims & documentation. For UK clinics, compile teleconsult notes + Rx decisions into a VetXML-ready pack for e-claims where relevant; in the US, prepare for payer documentation even without a unified standard.
Safe telemedicine flows (battle-tested patterns)
Advice-Only → Safety Net. Start with anamnesis, history, photos/video, and red-flag prompts; output documented advice plus a single-tap “Escalate to In-Person” when red flags or Rx-eligible intents appear (US: no new VCPR by video). The app saves time without crossing the prescribing line.
Triage → Channel Router. A rules engine (species, complaint, vitals, history, jurisdiction) decides if the session can stay remote, must convert to in-person, or needs emergency referral. In the UK, allow remote Rx only when the medicine class and the vet’s clinical assessment permit; otherwise require a physical exam before enabling eRx.
Existing VCPR Continuity (US). Where a VCPR already exists, enable follow-ups and refills consistent with federal/state law—still block first-time VCPR creation remotely and surface “refill-eligibility” logic directly in the UI (e.g., time since last PE, condition trajectory, lab results).
Remote Prescribing with 24/7 Follow-Up (UK). Enforce the RCVS requirement that any vet taking an animal “under care” must ensure round-the-clock ability to examine in person (directly or via formal arrangements). The app should verify such arrangements exist before enabling remote POM-V prescribing.
Controlled Drugs & Quantities (UK). For controlled drugs, prompt for physical exam confirmation and default to short supply (e.g., ~30 days) unless a documented justification is entered, aligning with RCVS/VMD guidance.
Privacy & data boundaries your UX must reflect
HIPAA does not cover vets, but many US states impose veterinary record-confidentiality statutes. Treat owner data as personal data (consent, access, breach notifications), and avoid implying HIPAA compliance in marketing unless you truly act as a business associate to a covered entity (rare in small-animal practice). In the UK, UK GDPR applies to client personal data; data about the animal is not itself “personal data,” but owner identifiers in clinical records plainly are—engineer for subject access and lawful bases accordingly.
Why this matters for delivery
Regulatory drift is real: states revisit telemedicine allowances; the UK CMA’s remedies may force price disclosures, generic prescribing, and clearer Rx options in 2025–26. If you hard-code those rules into your vet app development from day one—jurisdiction toggles, Rx class checks, audit trails, and disclosure UI—you ship faster, avoid rework, and build trust with clinicians and owners.
A-Bots.com bakes these controls into the architecture: jurisdiction-aware feature flags, medication-class gating for UK flows, US VCPR enforcement, PIMS-level status checks before eRx, and WORM audit ledgers. That’s how compliance becomes an enabler of great telehealth UX, not a blocker. vvca.org

3.Architecture Blueprint for Vet App Development: Mobile ↔ PIMS Data Spine, Offline-First Sync, Security & Audit
In vet app development, architecture is product. A beautiful UI that can’t honor PIMS reality, survive offline, or prove compliance will fail the first busy Monday. Below is a practical blueprint you can lift into your own backlog. It treats PIMS as the data spine, designs sync for bad networks, and bakes security/audit into every flow.
The Data Spine: canonical model over vendor APIs
Real work—appointments, SOAP, orders, charges—lives in PIMS. Your app should not mirror each vendor’s schema. Instead, create a canonical model and write thin adapters per PIMS:
-
Core entities: Owner, Animal, Encounter, Observation, Order (Labs/Imaging), Result, MedicationRequest/eRx, Claim, Charge, Message, Attachment.
-
Standards bridges:
- Export/interop via HL7 FHIR (use the Patient-animal extension: species, breed, reproductive status). This keeps “download my records” and referrals portable without locking you to a single vendor.
- In the UK, map admin/claims to VetXML/VetEnvoy to reach insurers and allied services with status tracking. vetxml.co.uk
Why this matters: PIMS schemas vary and evolve. A canonical model prevents “ripple rewrites” across your mobile clients and analytics when a vendor renames a field or ships a new module.
Event-Driven Integrations: webhooks in, REST/GraphQL out
Design event-first. Let PIMS tell you what changed; fetch details on demand; reconcile in a durable queue.
-
Provet Cloud exposes REST API plus webhooks (object + ID in the POST body; expects HTTP 200). That’s perfect for lightweight “wake-ups” to pull full records. developers.provetcloud.com
-
Vetspire runs on GraphQL, with developer docs, query libraries, and event/webhook concepts—excellent for selective reads and type-safe mutations. Vetspire, Vetspire Support
Pattern:
-
Webhook hits your Integration Service →
-
Service enqueues a job with idempotency key
{system}:{entity}:{id}:{version}→ -
Worker pulls full record via REST/GraphQL →
-
Transforms to canonical model →
-
Upserts to your Operational Store →
-
Emits app-level events (e.g.,
Encounter.Updated) to mobile subscribers.
Offline-First Sync: design for intermittent reality
Mobile vet teams work in basements, barns, shelters, vans. Your vet app development must assume no signal:
-
Local store: encrypted SQLite per user + content-addressed attachments (photos, PDFs, DICOM links).
-
Operation logs, not diffs: record user intents (
CreateEncounter,AddCharge,AttachPhoto). -
Idempotency & conflict policy:
-
Use stable client IDs (
cid) so retries don’t duplicate. -
Resolve conflicts by field-level merge with server timestamps; where clinical risk exists (e.g., meds, charges), force human resolution with a compare view.
-
-
Back-pressure: when PIMS rate-limits, drain your queue gradually; never drop clinical writes.
-
Graceful degradation: if jurisdiction blocks eRx (e.g., no VCPR), keep Advice-Only and Book In-Clinic working offline; sync the decision trail later.
eRx & Pharmacy Rails: integrate the networks you’ll actually use
Prescribing isn’t a custom endpoint; it’s a network choreography. Your Integration Service should support multiple rails and select per clinic/market:
- Surescripts e-prescribing (including EPCS for controlled substances) underpins retail fulfillment at scale in the US; treat it as a first-class rail alongside in-house pharmacy and mail-order partners. Use status callbacks to keep the chart and owner app in sync. Surescripts
Guardrails in code: jurisdiction checks (no new VCPR by video), drug-class blocks, refill eligibility, and accountable overrides must live in the same policy engine that gates UI actions.
Security by Construction: least privilege, zero trust inside the clinic
-
Scoped credentials per integration. Use vendor-issued app credentials (e.g., Provet Cloud Open API access creates a virtual user & permission group) so every call is attributable and revocable. support.provet.cloud
-
Role-based UI: Owner vs. Vet vs. Tech vs. Front Desk see different actions; hide “Sign & Send” unless policy engine allows it.
-
Secrets & storage: platform KMS for keys; app secrets in OS keystores; all local DBs encrypted; attachments chunked & checksummed.
-
Network posture: mutual TLS between mobile and Integration Service; vendor APIs over TLS with cert pinning where feasible.
-
PII boundaries: remember: vet records aren’t HIPAA by default, but client data is personal data (GDPR in UK); build subject-access export endpoints early.
WORM Audit & Observability: make every clinical action provable
-
WORM event log: append-only records for advice given, orders placed, eRx attempts (allowed/blocked), charge edits, consent; hash-chain batches to a tamper-evident ledger.
-
SLOs that matter:
-
PIMS data freshness (p95): ≤ 15 s from vendor webhook to app view
-
eRx round-trip (p95): ≤ 60 s to external network ACK
-
Offline write durability: 0 lost ops across app restarts/power loss
-
-
Red/Amber rules: if lab result → treatment estimate delta > threshold, raise a “review-required” banner until acknowledged.
Reference Topology (words instead of a diagram)
Mobile Apps (Owner, Staff) ↔ API Gateway ↔ Integration Service (adapters: Provet, Vetspire, Labs, eRx, Payments, Claims) ↔ Operational Store (canonical model) ↔ Event Bus (to push deltas back to devices) ↔ Long-term Warehouse (analytics, quality, cohorting).
Policy Engine (jurisdiction, drug-class, VCPR/‘Under Care’) and Audit Ledger cut across all paths.
Build Notes you can copy into tickets
- PIMS adapters: start with Provet Cloud (REST + webhooks) and Vetspire (GraphQL), then add others; keep transformer functions pure and versioned.
- Sync: one queue per entity type; exponential backoff;
If-Match/versionheaders where vendor supports; otherwise optimistic concurrency + conflict UI. - Attachments: upload before metadata commit; show placeholder with retry.
- Claims (UK): emit VetXML packs and post through VetEnvoy where supported; store carrier responses as immutable documents. vetxml.co.uk
- eRx: abstract order routes so clinics can switch between in-house/retail rails without UI changes; surface network errors to staff with suggested next steps.
Why this blueprint wins
-
Clinicians get truth, not copies. The app reflects PIMS minutes after changes and survives no-signal fieldwork.
-
Compliance is encoded, not narrated. Jurisdiction & drug-class logic live in code paths that gate actions.
-
Change-tolerant by design. Vendor APIs can evolve without forcing mobile rewrites.
A-Bots.com implements this blueprint as reusable playbooks—PIMS adapters (Provet Cloud, Vetspire, others), a hardened Integration Service, offline-first sync modules, and a policy/audit core. That’s how vet app development ships from MVP to multi-clinic scale without re-architecture.
4.Features That Move the Needle: Client App, Staff App, Telemedicine, eRx, Claims, Imaging/PACS & AI Scribe—Prioritized by Outcomes
Most feature lists read like wishful thinking. In vet app development, the only features that matter are those that reduce clinical friction, capture revenue you already earn, or prevent regulatory missteps. Below is a pragmatic, outcome-first catalog you can plug into roadmaps and dashboards.
Client App (pet owners): reduce attrition, no-shows, and checkout friction
What to ship
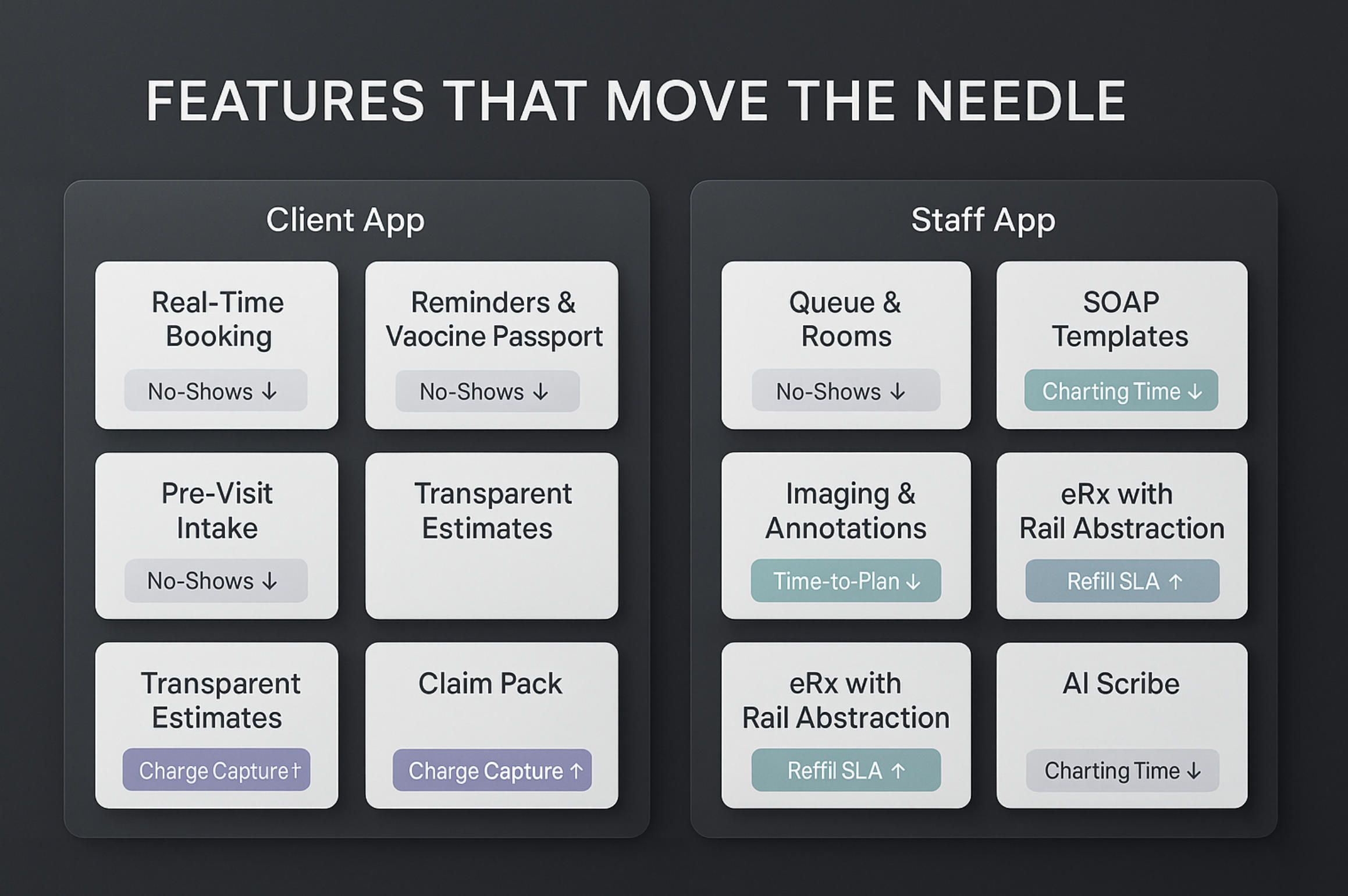
- Real-time booking that honors PIMS rules (provider, slot length, visit reason) and shows earliest viable appointments without back-and-forth.
- Reminders & vaccination passport (push/SMS/email) with one-tap add-to-calendar and a readable vaccine card for travel/daycare use.
- Self-serve forms & pre-visit intake (history, diet, meds, photos, video) to shorten anamnesis time.
- Estimates & transparent pricing tied to the chart; pre-authorizations and financing rails (CareCredit/Scratchpay or clinic-preferred) before the visit.
- Claims pack generator (UK: VetXML pack; US: document bundle) prepared from the encounter and attachments.
- Two-way messaging with templated quick-replies from staff to keep owners informed without phone tag.
Why it moves the needle
- No-show rate↓, rebook speed↑, owner NPS↑, ARPC (avg. revenue per client)↑ via pre-approved care plans and financing.
- Time-to-checkout↓ by collecting signatures and payments in-app.
Instrumentation
- No-show% before/after, rebook_time_p50/p90, % appointments self-scheduled, pre-auth rate, financing uptake, claim-ready%.
Staff App (technicians & vets): capture charges, compress cycle time, minimize double entry
What to ship
- Queue view (patients in building / in room / lab pending / discharge ready) with color codes driven by PIMS status.
- Structured SOAP templates with breed/species defaults; barcode/QR scanning for meds and inventory.
- Charge capture at point of care (procedures auto-attach charges; “estimates→actuals” reconciliation prompts).
- Photo/video capture that auto-tags the encounter and stores hashes for chain-of-custody (WORM-ready).
- Offline-first operation with conflict resolution on meds/charges.
Why it moves the needle
- Missed charges↓ (leakage often hides in add-ons and consumables), charting time↓, throughput↑ per clinician hour.
Instrumentation
- Charge capture delta = (billed_before − billed_after)/billed_before, median charting time, procedures per hour.
Telemedicine (triage & follow-ups): expand access without crossing legal lines
What to ship
- Advice-only flow distinct from diagnose/prescribe, with red-flag checklists and structured dispositions (stay remote → in-clinic → ER).
- Jurisdiction gates (US: no first-time VCPR via video; UK: “Under Care” + drug-class checks).
- Refill eligibility logic (existing VCPR only; time since PE; condition stability).
- Owner consent & disclosures (pricing/options) presented contextually, not buried.
Why it moves the needle
- Phone tag→structured triage, conversion to in-clinic↑ for red flags, risk↓ from out-of-bounds eRx attempts.
Instrumentation
- % advice-only vs. Rx-eligible, triage→visit conversion, blocked eRx attempts (policy), median wait to live consult.
eRx & Pharmacy: orchestrate the networks you’ll actually use
What to ship
- Formulary-aware prescribing with clinic defaults, weight-based calculators, and hard stops for controlled classes where required.
- Rail abstraction: in-house → mail-order → retail (Surescripts) or partner (Vetsource/Covetrus) without UI changes.
- Refill workflows with status callbacks into the chart and client app.
- Auto-attach charges for dispensing/labeling when pharmacy is in-house.
Why it moves the needle
- Refill turnaround↑, leakage↓ (fewer lost scripts), rework↓ from mis-keyed orders, owner satisfaction↑.
Instrumentation
- eRx ACK p95, refill SLA meet%, script leakage to external retail, error rate (dose/strength/quantity mismatches).
Claims (UK today, US tomorrow): shrink admin drag, speed payouts
What to ship
- VetXML document packs compiled from the encounter (diagnosis, codes, estimates, invoices, labs, imaging notes) and transmitted via the clinic’s channel.
- Status ingestion into the staff and owner apps (submitted → query → approved → paid).
- US-ready pack generator (PDF bundle + metadata) to ease manual carrier portals while the market standardizes.
Why it moves the needle
- Admin time↓, payout speed↑, and owner trust↑ when status is transparent.
Instrumentation
- time_to_submit, time_to_decision, insurer queries per claim, owner calls about status/week.
Imaging/PACS on mobile: shorten diagnostic loops, improve referrals
What to ship
- DICOM viewer with basic window/level presets and measurement tools; hyperlinks back to the chart.
- Capture→order linking so every image has an order and a charge; annotated exports for referrals.
- Result-driven tasking: abnormal imaging auto-creates a review/estimate task for follow-up.
Why it moves the needle
- Time-to-plan↓ after imaging, missed follow-ups↓, referral collaboration↑.
Instrumentation
- median minutes: image available → plan created, unreviewed imaging >24h, referral package completeness%.
AI Scribe & Dictation: return minutes to clinicians, raise documentation quality
What to ship
- Ambient or push-to-talk dictation with medical vocabulary tuned for species/breeds.
- SOAP auto-drafts with highlight/accept editing; reason codes for changed suggestions to build a learning loop.
- Template learning: suggest plan items based on diagnosis + lab results; guardrails to avoid over-automation.
Why it moves the needle
- Charting time↓ 20–40% in typical deployments, note completeness↑, burnout risk↓.
Instrumentation
- median minutes per SOAP, % reused templates, accept/edit ratio, late charts.
Prioritization by outcomes (what to build first)
Phase 0 — Instrumentation before features.
Set up event logging and a baseline dashboard: no-show%, charge capture, charting time, refill SLA, imaging review time. Without a baseline, you can’t claim impact.
Phase 1 — Throughput & revenue protection.
Ship Staff App (charge capture, SOAP, queue) + Client App (booking, reminders, intake). These two alone typically cut leakage and wait times.
Phase 2 — Orchestration rails.
Add eRx abstraction and Imaging/PACS hooks; your app now operates across the core clinical loop.
Phase 3 — Admin efficiency & AI.
Enable Claims packs (UK first), then AI Scribe for sustainable charting speed.
Anti-patterns to avoid (they quietly destroy outcomes)
- “Copy-the-PIMS” data model. When vendor schemas change, your mobile app breaks. Use a canonical model with adapters.
- One giant “telehealth” button. Without advice-only vs. Rx-eligible separation and jurisdiction gates, you invite violations.
- Uploads without order linkage. Images and lab photos must map to orders and charges, or you leak revenue and context.
- Offline as an afterthought. If your queue can drop writes on app restarts, clinicians will never trust mobile.
A-Bots.com delivers these as integration playbooks (PIMS adapters, eRx rails, claims packs), offline-first sync, and policy/audit modules. You get the features that actually move the needle—shipped on an architecture that survives Mondays.
5.Delivery & TCO: Integration Playbooks, SLOs, and a Cost Model You Can Reuse
In vet app development, you don’t buy features—you buy time-to-outcome under regulatory and integration constraints. This section gives you a delivery blueprint you can hold a vendor to, plus a transparent TCO model you can adapt to your clinic or network.
Integration playbooks (the “how” you can actually ship)
Why playbooks? Because PIMS, labs, eRx, payments, and claims each have their own auth models, rate limits, and event semantics. Codifying them as playbooks turns “unknown unknowns” into estimable work.
Core playbooks we bring to projects
- PIMS adapters. Canonical data model (Owner, Animal, Encounter, Order, Result, MedicationRequest, Claim, Charge, Message, Attachment) + thin vendor mappers; event-first ingestion (webhooks → durable queue → fetch-by-ID → transform → upsert).
- Labs & imaging. Orders with catalog validation, result polling/callbacks, attachment hashing, DICOM deep links, and “order↔charge” reconciliation to eliminate leakage.
- eRx rails. Formulary-aware prescriber UX, rail abstraction (in-house vs. partner vs. retail), refill eligibility logic, controlled-drug gates, status callbacks to chart and client app.
- Claims & admin. UK: VetXML pack assembler and status consumption; US: claim bundle generator (PDF + metadata) with carrier-specific notes to reduce rework.
- Payments & financing. Pre-auth flows tied to estimates, post-care settlements, and financing options surfaced before treatment.
- Policy & audit. Jurisdiction switches (US VCPR, UK “Under Care”), advice-only vs. prescribe flows, WORM event log across advice, orders, eRx attempts (allowed/blocked), and consents.
Each playbook ships with: scope, sequence diagram, error taxonomy, rate-limit strategy, security notes, and a test plan (unit, contract, and sandbox end-to-end).
Delivery phases & concrete artifacts (what you get, not just “we’ll be agile”)
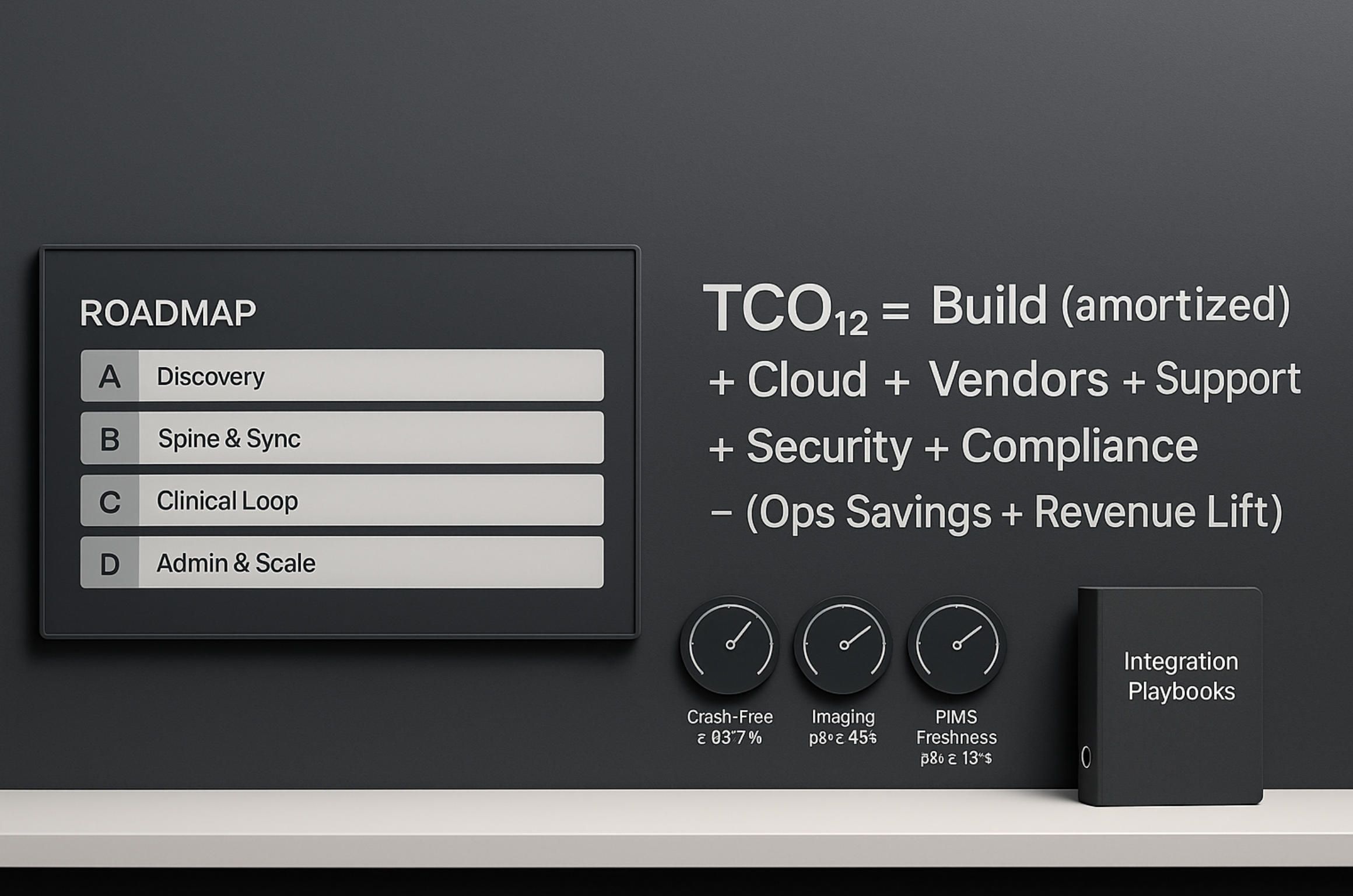
Phase A — Discovery (2–4 weeks, time-boxed).
Deliverables: integration matrix (systems, endpoints, limits, SLAs), data contracts (canonical schema + vendor deltas), jurisdiction policy map (US/UK baseline), security posture (roles, scopes, storage), observability plan (logs/metrics/traces). Outcome: fixed scope for MVP with risk register.
Phase B — Spine & sync (4–8 weeks).
Deliverables: Integration Service, Operational Store, event ingestion, offline-first mobile scaffolding, initial PIMS adapter, basic dashboards for freshness and error budgets. Outcome: the product has a heartbeat; data round-trips end-to-end.
Phase C — Clinical loop (4–8 weeks).
Deliverables: Staff App (queue, SOAP, charge capture), Client App (booking, reminders, intake), labs ordering/results, imaging deep links, eRx rail #1, policy engine v1. Outcome: a usable clinic loop that survives Mondays.
Phase D — Admin & scale (4–8 weeks).
Deliverables: claims packs (UK first), payments/financing, eRx rail #2, AI scribe, SSO/MFA, audit ledger, cost and performance tuning. Outcome: measurable admin time reduction and consistent throughput.
A-Bots.com runs these phases with weekly demos, signed exit criteria, and change control for anything new that emerges (we prefer to be asked to slow down rather than to “be more transparent”).
SLOs that matter (and the error budgets behind them)
SLOs convert “quality” into yes/no. Below is a default set we negotiate; you’re free to raise/lower targets to match your risk appetite.
- PIMS data freshness (p95): ≤ 15 s from vendor event to staff/owner view.
Error budget: ≤ 5% events breaching 15 s in any rolling 7-day window. - Offline write durability: 0 lost operations across app restarts and power loss (verified by chaos tests weekly).
- eRx network ACK (p95): ≤ 60 s from “Sign & Send” to external ACK (if the rail is up).
Error budget: ≤ 1% eRx attempts retry-queued > 5 min. - Imaging availability (p95): ≤ 45 s from acquisition to link in chart.
- Crash-free sessions (mobile): ≥ 99.7% monthly.
- Telemetry delay (owner messaging): ≤ 10 s p95 for inbound/outbound delivery.
- Policy enforcement accuracy: 100% for jurisdiction and drug-class gates in regression suite; 0 critical false-negatives in production.
Each SLO has a runbook: symptoms, likely causes (rate limit, webhook backlog, vendor outage), mitigation (drain strategy, degraded mode), and on-call ownership.
Cost drivers (so you can predict, not guess)
One-time (CapEx-like)
- Integrations. Number and depth of PIMS/lab/eRx/claims/payments connectors; availability of sandbox; need for custom data bridges.
- Mobile scope. Client App vs. Staff App, imaging viewer, AI scribe footprint, offline complexity, accessibility and localization.
- Security & compliance. SSO/MFA, WORM ledger, data retention/export (e.g., FHIR), audit scope, pen test remediation.
- Change management. Content (templates, forms), training, and go-live support across sites.
Recurring (OpEx)
- Cloud & observability. Compute, storage, CDNs, observability (traces/logs), attachment retention.
- Vendor/API fees. eRx rails, payment processors, claims networks, voice/notifications.
- Support & maintenance. On-call, patching, API evolution, new-state rule updates.
- Model & content. AI scribe usage, medical vocabularies, prompt tuning.
Reusable TCO model (plug your numbers in)
Define your annualized TCO for vet app development as:
TCO12=Cbuild+Ccloud+Cvendors+Csupport+Csecurity+Ccompliance−Vops_savings+Vrev_lift
Where:
- Cbuild — discovery, spine, adapters, mobile apps, policy/audit (amortize over 3 years if you prefer).
- Ccloud,Cvendors,Csupport,Csecurity,Ccompliance — annualized recurring.
- Vops_savings— time saved on charting/admin, fewer calls about claim status, fewer manual uploads.
- Vrev_lift — reduced no-shows, better charge capture, faster refills, improved follow-up conversion.
Worked example (conservative)
-
Clinic with 4 doctors, ~25 visits/doctor/day ⇒ 100/day.
-
No-shows drop from 8% to 5% due to self-booking + reminders: that is 3 regained visits/day.
If ARPC = $160, regained revenue/day = 3×160=480.
For 22 working days, monthly regain = 480×22=10,560. -
Charge capture: if monthly billings $240,000, leakage 4% = $9,600; halving leakage recovers $4,800/month.
-
AI scribe: saves 0.6 h/doctor/day (30% of a 2-hour charting block). For 4 doctors: 0.6×4=2.4 h/day.
At a burdened rate $90/h: 2.4×90=$216/day; monthly 216×22=$4,752. -
Total monthly benefit: 10,560+4,800+4,752=20,112.
-
Monthly run-rate costs: cloud $1,200 + vendor APIs $600 + support $2,000 ⇒ $3,800.
-
Net monthly impact: 20,112−3,800=16,312.
-
If build cost = $180,000, payback ≈ 180,000/16,312≈11.0 months.
Swap in your numbers; the model holds.
Acceptance criteria you can put in the contract
- Data freshness meets SLO for 14 consecutive days prior to go-live; backlog drains < 10 minutes after vendor outage drills.
- Offline-first verified by scripted flight-mode scenarios for all clinical writes (encounter, charges, notes, photos).
- Policy gates block 100% out-of-bounds eRx attempts in staging with jurisdiction toggles; no critical regressions in production.
- Claims packs generated for 10 consecutive UK test cases with carrier acceptance; US bundles pass clinic audit.
- Crash-free ≥ 99.7% over 30 days on supported OS versions.
- Observability: live dashboard for SLOs; alert routes tested; on-call runbooks acknowledged by clinic champion.
How A-Bots.com executes (quietly, so it scales)
We build once and reuse the right parts: integration playbooks, offline-first sync, policy/audit core, and mobile scaffolds. You get predictable time-to-first-value and a TCO you can defend to finance. If you’re evaluating partners for vet app development, start with this section: copy the SLOs and the TCO equation into your RFP. We’ll happily respond against them.
6.Build-to-Scale with A-Bots.com: Engagement Models, Case-Style Patterns & a Vet App Development RFP Checklist
In vet app development, scale comes from disciplined delivery, not from feature wishlists. This section shows how A-Bots.com engages, what patterns repeatedly work across clinic types, and a reusable RFP checklist that forces vendors (including us) to commit to measurable outcomes—not promises.
Engagement models (pick the cadence that fits your risk & timeline)
Model A — Discovery-to-Decision (2–4 weeks, time-boxed).
For leaders who want clarity before code. You get: an integration matrix (PIMS, labs, eRx, claims, payments), a canonical data schema with vendor deltas, a jurisdiction policy map (US VCPR / UK “Under Care”), a security posture (roles, scopes, storage), SLO targets, and a budget/timeline with risks. Output: a go/no-go package board can approve.
Model B — Fixed-Scope MVP (10–16 weeks, acceptance criteria signed).
A production-ready slice: Staff App (queue, SOAP, charge capture), Client App (booking, reminders, intake), one PIMS adapter, labs ordering/results, eRx rail #1, policy gates. Ship with dashboards for data freshness and error budgets. Acceptance criteria mirror the SLOs you set.
Model C — Integration-First Spine (adapters before UX).
For groups with messy estates or multiple PIMS. We implement the Integration Service, canonical store, and event pipelines first, then layer mobile UX. This reduces rework and is the safest path when vet app development must coexist with legacy tools.
Model D — Dedicated Product Squad (quarterly increments).
A long-running team with shared KPIs (no-shows, charge capture, charting time, refill SLA). Quarterly objectives; monthly demos; feature flags for safe rollout across sites.
Model E — Co-Development with Internal IT.
We keep adapters, offline sync, and policy/audit as shared libraries; your team owns selected screens or modules. Knowledge transfer is baked into the plan.
Governance you’ll actually feel: weekly demos, change control for scope shifts, on-call runbooks, and a single artifact room (architecture notes, test plans, SLO dashboards). You always see what is done, what is next, and how it performs.
Case-style patterns (the moves that keep working)
A) US multi-site small-animal group
PIMS mix, high phone volume, inconsistent refills. We lead with Staff App + Client App, then add eRx rail abstraction and AI scribe. Typical impact ranges: no-shows ↓ 20–40% relative, charge leakage ↓ 30–60% relative, median charting time ↓ 20–40%.
B) UK corporate with insurance exposure
Heavy VetXML/VetEnvoy usage, CMA-driven transparency. We ship claims packs + status in owner app, price disclosures, and UK prescribing gates (antimicrobials/controlled drugs). Outcome: faster payouts, fewer status calls, cleaner audit.
C) Specialty/referral hospital
Imaging-centric flow, complex estimates. We implement DICOM deep links, result-driven tasks, and “estimates→actuals” reconciliation. Outcome: time-to-plan after imaging shrinks; referral packages are complete by default.
D) Mobile/field/farm practice
Unreliable connectivity. We deploy offline-first sync with operation logs, conflict UI for meds/charges, and photo/video capture tied to encounters. Outcome: zero lost writes; staff trust the app in barns and vans.
E) Shelter/rescue network
High intake, vaccine drives, grants. We prioritize batch intake, vaccine passport at scale, and export/reporting endpoints. Outcome: less spreadsheet churn, faster grant reporting, better adopter comms.
These patterns aren’t “case studies for a slide”—they’re delivery playbooks we reuse and adapt. That’s why our vet app development remains predictable as scope grows.
The Vet App Development RFP checklist (copy-paste for vendors)
Business outcomes & KPIs
- Target deltas for: no-shows, charge capture, charting time, refill SLA, imaging review latency, claim time-to-decision.
- Baseline measurement plan and dashboards before feature launch.
PIMS & data spine
- Named PIMS (e.g., Cornerstone/Neo/ezyVet, Provet Cloud, Vetspire, Digitail, Shepherd, AVImark/ImproMed/Pulse) and expected read/write scope.
- Canonical model vs. vendor schema; event-driven ingestion; webhook strategy; idempotency keys; conflict resolution policy.
Labs & imaging
- Orders, catalog validation, results callbacks; attachment hashing and DICOM links; “order↔charge” reconciliation; abnormal-result tasking.
Telemedicine & compliance
- US: VCPR enforcement (no first-time VCPR over telemedicine), advice-only vs. Rx flows, refill eligibility rules.
- UK: “Under Care” gates for POM-V; drug-class prompts (antimicrobials/controlled drugs), 24/7 in-person follow-up arrangements surfaced in UI.
- Consent & disclosure UX; WORM audit for advice, eRx attempts (allowed/blocked), overrides with reason codes.
eRx & pharmacy rails
- Rail abstraction (in-house, partner networks like Vetsource/Covetrus, retail via Surescripts), status callbacks, controlled-substance handling, label/dispense charging.
Claims & admin
- UK: VetXML pack generation + status ingestion (VetEnvoy or clinic channel).
- US: claim bundles (PDF + metadata) with carrier notes; plan for future standardization.
Payments & financing
- Pre-auth tied to estimates; post-care settlement; options for CareCredit/Scratchpay; reconciliation into PIMS.
Offline-first requirements
- Local encrypted store; operation logs; back-pressure handling; conflict UI for meds/charges; chaos tests for power loss and app restarts.
Security & privacy
- RBAC, scoped vendor credentials, MFA/SSO, mobile keystores, data retention, export (FHIR) and admin portability (VetXML), breach procedures.
Observability & SLOs
- PIMS freshness p95 ≤ 15 s; eRx ACK p95 ≤ 60 s; imaging availability p95 ≤ 45 s; crash-free ≥ 99.7%; message delivery p95 ≤ 10 s; 0 lost writes offline.
- Error budgets, alert routes, and runbooks owned by named roles.
QA & acceptance
- Contract tests for each integration, sandbox credentials, UAT scripts per role (Owner/Vet/Tech/Front Desk), cut-over plan, and rollback.
Support & lifecycle
- On-call hours and response targets, API change management, state-rule updates cadence, release train, feature flags & staged rollout.
Commercials & TCO
- Build vs. run-rate split; vendor/API fees listed; instrumentation for realized benefits; quarterly TCO/ROI reports.
If a bidder can’t (or won’t) answer each bullet in writing, they are asking you to fund their discovery.
Why A-Bots.com
- Integration playbooks on day one. We bring PIMS adapters, lab/eRx connectors, offline-first sync, and policy/audit rails as reusable modules—fewer unknowns, faster first value.
- SLOs instead of slogans. We sign up to freshness, durability, and crash-free targets, with dashboards you can see.
- Architecture you can own. Canonical data model, export via FHIR, UK VetXML packs, and a tameable cost structure—so your vet app development isn’t a black box.
- Change without chaos. Feature flags, staged rollouts, and on-call runbooks; compliance gates live in code, not in PDF manuals.
If you already have an RFP, send it. If not, paste the checklist above into a document, add your priorities, and we’ll respond with a scoped plan, timeline, and a TCO you can defend to finance. A-Bots.com is IoT Application Development Company.
FAQ — Vet App Development
1) What exactly falls under “vet app development” in 2025?
Building mobile apps that plug into a clinic’s real systems of record—PIMS, lab & imaging rails, e-prescribing networks, payments, and (in the UK) insurance claim flows—while enforcing jurisdiction-specific telemedicine rules (US VCPR, UK RCVS “Under Care”). It’s not a standalone UI; it’s an integration product.
2) Which PIMS should we target first?
Pick what your clinics actually use and what exposes workable APIs: Provet Cloud (REST + webhooks), Vetspire (GraphQL), IDEXX stack (Cornerstone/Neo/ezyVet via partner pathways), Digitail/Shepherd, or Covetrus family (Pulse/AVImark/ImproMed). Start with one high-leverage adapter and expand.
3) Can a US clinic establish a VCPR over video?
No. At the federal level you cannot establish a VCPR solely via telemedicine. Design the app to block first-time VCPR creation remotely and route owners to in-person visits.
4) How is the UK different under RCVS “Under Care”?
Remote prescribing can be allowed after a clinical assessment, but certain classes (e.g., antimicrobials/controlled drugs) typically require a physical exam. Your app should gate prescribing based on drug class and the vet’s assessment.
5) Do we need a separate “client app” and “staff app”?
Yes. Owners need booking, reminders, intake, payments, and claim status; staff need queue/room views, SOAP, charge capture, labs, imaging, and eRx. Mixing both into one UI increases cognitive load and data-leak risk.
6) How do we make offline work reliable for mobile/field teams?
Use an encrypted local store, operation logs (not diffs), idempotent writes with stable client IDs, and conflict UIs for risky entities (meds/charges). Never drop writes on app restarts.
7) What’s the fastest way to avoid “double entry” hell?
Adopt a canonical data model (Owner, Animal, Encounter, Order, Result, MedicationRequest, Claim, Charge, Message, Attachment) and map each PIMS to it via thin adapters. Consume vendor webhooks, fetch by ID, transform, upsert.
8) Can we export data without vendor lock-in?
Yes. Emit FHIR resources for portability (patient-animal extension) and VetXML for UK insurer/admin exchanges. Keep exports first-class, not one-off scripts.
9) How should e-prescribing be implemented?
Treat eRx as a rail abstraction: in-house dispensing, partner networks (e.g., Vetsource/Covetrus), and retail via national networks. Add formulary checks, weight-based calculators, refill eligibility, and jurisdiction/controlled-drug gates.
10) What imaging/PACS capabilities belong on mobile?
Deep links to DICOM studies, basic viewer with measurements, annotations that round-trip to the chart, and auto-creation of review/estimate tasks when abnormal results arrive.
11) How do we prevent missed charges?
Tie procedures to charge sets in the Staff App, reconcile estimates→actuals, and require charge review on discharge. Show a “charge delta” banner whenever labs/imaging generate downstream items.
12) What SLOs should we hold a vendor to?
Examples: PIMS freshness p95 ≤ 15s; eRx ACK p95 ≤ 60s; imaging availability p95 ≤ 45s; crash-free ≥ 99.7%; message delivery p95 ≤ 10s; 0 lost offline writes. Each SLO needs an error budget and runbook.
13) Is HIPAA relevant to veterinary apps?
Generally no—HIPAA covers human healthcare. Still, owner data is personal data (privacy laws apply), and you should engineer for consent, subject-access requests, and secure storage.
14) How do we price and forecast TCO?
Use a build-vs-run model: amortized build (spine, adapters, apps, policy/audit) + cloud + vendor fees + support + security/compliance − (ops savings + revenue lift). Track benefits using no-show%, charge capture, charting time, refill SLA, and claim cycle time.
15) What’s a realistic MVP scope for vet app development?
Staff App (queue, SOAP, charge capture), Client App (booking, reminders, intake), one PIMS adapter, labs ordering/results, one eRx rail, and policy gates. Ship observability from day one.
16) How do we handle UK insurance today and the US tomorrow?
UK: generate VetXML packs and ingest statuses (submitted→approved→paid). US: produce standardized claim bundles (PDF + metadata) to reduce manual rework while the market converges.
17) What about payments and financing?
Surface pre-authorizations tied to estimates, post-care settlement, and financing offers (e.g., CareCredit/Scratchpay) before treatment to minimize counter surprises and improve conversion.
18) Can AI scribe actually save time?
Yes, when embedded at the point of care with SOAP auto-drafts, highlight-to-accept editing, and species-aware vocabulary. Measure impact as median minutes per SOAP and late-chart counts.
19) How do we keep telemedicine safe instead of risky?
Separate advice-only from diagnose/prescribe flows; enforce jurisdiction gates (US VCPR, UK drug-class rules); preface every session with consent/disclosures; and log everything to a WORM audit.
20) What’s the right approach to security?
RBAC by role (Owner/Vet/Tech/Front Desk), scoped vendor credentials, MFA/SSO, encrypted local stores, mutual TLS, retention policies, and breach procedures. Attribute every external call to a virtual user or service account.
21) How do we de-risk multi-PIMS estates?
Implement the Integration Service and canonical store first, then add adapters incrementally. Keep transformers versioned and pure; don’t leak vendor fields into app code.
22) Which metrics actually prove value to stakeholders?
No-show rate, rebook speed, charge capture delta, median charting time, eRx turnaround, imaging review latency, claim time-to-decision, owner NPS, and crash-free rate.
23) How should releases roll out across clinics?
Feature flags per site/role, staged rollout (1%→10%→25%→100%), crash and SLO guards, and automatic rollback when error budgets are burned.
24) What accessibility and localization should we plan for?
WCAG-minded UI (contrast, text size, semantic controls), haptic/voice assist for staff in gloves, and localization for owner-facing screens (date/number formats, units, species/breed names).
25) How do we test integrations without risking production?
Use vendor sandboxes where available; otherwise, contract tests plus “shadow mode” that reads production safely and writes to a quarantined store. Run chaos drills for webhook backlogs and vendor rate limits.
26) Why A-Bots.com for custom vet app development?
We bring reusable integration playbooks (PIMS adapters, labs/eRx connectors), offline-first sync, policy/audit rails for VCPR/RCVS, SLO-backed delivery, and a TCO model finance can sign off on—so your project reaches outcomes faster and scales cleanly.

✅ Hashtags
#VetAppDevelopment
#VeterinarySoftware
#PIMS
#ezyVet
#IDEXX
#ProvetCloud
#Vetspire
#eRx
#Telemedicine
#RCVS
#VCPR
#VetXML
#VetEnvoy
#DICOM
#AIBased
#MobileHealth
#PetCareTech
#ABots
Other articles
Mobile App Development for Smart Pet Feeders Smart pet feeders are no longer luxury gadgets — they are becoming vital tools in modern pet care. But their true power is unlocked only through intuitive, connected mobile apps. This article explores how custom software development elevates the user experience far beyond off-the-shelf solutions. From feeding schedules to AI-driven health monitoring, we break down what pet owners truly expect. We analyze the market, dissect real product cases, and outline the technical architecture behind dependable smart devices. Most importantly, we show why hardware manufacturers need the right digital partner. A-Bots.com delivers the kind of app experience that builds trust, loyalty, and long-term value.
Custom Mobile App Development for Smart Dog Collars The future of pet care is connected—and mobile apps are at the heart of it. This article explores how smart dog collars are evolving into real-time safety hubs, with integrated GPS, cameras, microphones, and LED displays. We analyze the global pet-tech boom and explain why software, not just hardware, drives loyalty and recurring revenue. You'll discover what pet owners want, what competitors miss, and how custom mobile apps turn simple sensors into premium services. A-Bots.com reveals the technical and UX patterns that create trust, conserve battery, and unlock delight. From bark detection to programmable LED scrolls, the app is where peace of mind happens. Learn how we help manufacturers lead the pack.
Pet Hotel App Development Running a pet hotel today means juggling occupancy spikes, exact-time medication, anxious pet parents, and ever-stricter compliance rules. In this in-depth guide, A-Bots.com—an award-winning pet care app development company—details a battle-tested architecture that ties Flutter guest apps, Kafka-powered micro-services, edge IoT sensors, and zero-trust security into one seamless ecosystem. Learn how real-time pricing, NFC proof-of-care, and AI shift scheduling lift margins; see why modular Kubernetes and serverless functions keep cloud spend under 4 % of booking value; and get a 12-month roadmap that scales from single-site MVP to global franchise. Whether you operate a boutique cat condo or a multi-property boarding chain, this article maps every technical and operational step toward a lovable, revenue-rich pet-hotel empire.
ShelterHeart: Crowdfunded Pet Shelter App ShelterHeart is a next-generation mobile platform that bridges animal lovers and shelters through sponsorship, adoption and data-driven care. On the user side, supporters enjoy one-tap monthly donations, live health dashboards and even AR meet-and-greets with future furry friends. For shelters, an integrated Command Center replaces scattered spreadsheets with real-time inventory forecasts, AI adoption matching and grant-ready analytics. Architected by A-Bots.com on a fault-tolerant, microservice stack, the solution scales seamlessly from a single local rescue to a global, multi-tenant network—all while meeting GDPR, CCPA and veterinary compliance standards. The article outlines a phased crowdfunding strategy: seed a passionate community, validate demand with lightweight landing pages, then launch a tiered Kickstarter or Patreon campaign to finance the MVP. With transparent ROI metrics and white-label options, ShelterHeart empowers nonprofits to deploy life-saving technology without prohibitive upfront costs, turning every swipe into a tangible act of kindness.
Pet Product Delivery App Development This long-read maps how pet product delivery app development moves beyond “subscribe & save” into a data-first service. We show how to build nutrition-equivalency graphs that propose safe, breed- and condition-appropriate substitutes; orchestrate one cart across two regimes—raw or chilled foods and veterinary prescriptions—with thermal math, custody logs, and pharmacist workflows; and wire feeders, litter boxes, and fountains as sensors so reorders happen at the right hour with clear, human-readable justifications. The platform layer closes the loop with clinics, community resilience, and circular packaging pools that keep quality high during heat waves and peak demand. If you’re seeking a partner to take this from concept to launch, A-Bots.com can help—architecture, device SDKs, ops playbooks, and production-grade UX from a single mobile app development company. Start the conversation: https://a-bots.com/services/mobile
Custom Pet Care App Development This article maps how a mobile app development company like A-Bots.com approaches custom pet care app development as a platform, not a pile of features. We start with a Pet Identity Graph and Consent Ledger, layer multimodal Behavior AI from litter, feeders, wearables, and cameras, and then ship adaptive routines that keep working offline. Finally, we wire in the unglamorous but essential interoperability—FHIR bundles for clinics, claim-ready artifacts for insurers, AAHA-aligned microchip workflows, and shelter handoffs—so caregivers aren’t forced to be couriers. If you need custom pet care app development that’s trustworthy, explainable, and resilient in real life, this is the blueprint.
Top stories
Copyright © Alpha Systems LTD All rights reserved.
Made with ❤️ by A-BOTS